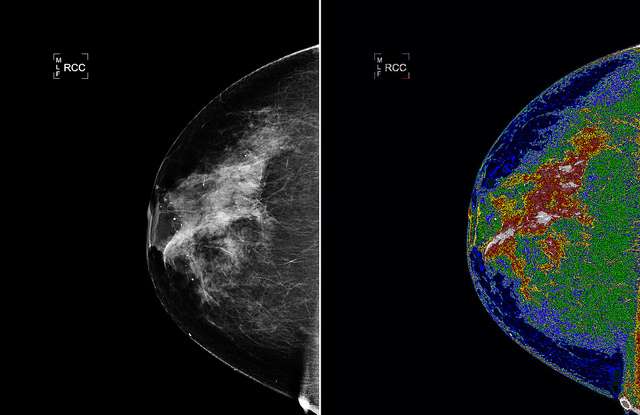
Detecting Breast Cancer Might Now Be Easier With Underwater Imaging Tech
A technique used for finding damage in underwater marine structures may be the most successful breakthrough in breast cancer detection yet.
Now that you've heard of ALS through the viral phenomenon known as the Ice Bucket Challenge, this southern California physician may have just discovered a more sure way of diagnosing – and treating – ALS.
Amyotrophic lateral sclerosis – or Lou Gehrig's disease – is an insidious neurodegenerative disease that attacks motor neurons which control volunteer bodily functions – like muscle use and breathing. It strikes about 0.8 to 8.5 people per 100,000 across the world with about 5% of these cases being linked to genetics, and the rest having many conjectured causes or triggers.
However one physician, David A. Steenblock from San Clemente, California, has a slightly different take on what triggers ALS and believes he has figured out the intricate web of players and pathways that contribute to ALS onset and fuels its progression. If he is right, a specific pattern of vertebral column injury and reinjury (which does not involve trauma to the spinal cord), followed by degenerative bone changes in the affected bones, is both trigger, player and biomarker for sporadic ALS in many sufferers.
In an interview published in the June 2016 issue of the Townsend Letter, Steenblock shared this:
"I believe that ALS is a complicated combination of unfortunate circumstances that occur sequentially. The first occurrence – for most cases – is a neck injury, perhaps caused by a fall, a collision on the sports field, whiplash, some kind of trauma that injures the cervical or neck vertebrae. This injury generally occurs many years before the onset of symptoms – perhaps in high school or shortly thereafter. The injury heals to a certain extent, but it also degenerates from wear and tear, so that, twenty or thirty years later, you see degenerative joint disease such as osteoarthritis and something called neuroforaminal stenosis (NFS), a narrowing of the spinal nerve canal often with calcium deposits around that spinal nerve. It takes many years of chronic irritation for this constriction to occur. So, over time, you're seeing an increase in the amount of extracellular calcium in and around the affected spinal nerve. At some point, years later, there's a re-injury of the same area"
Emboldened by decades of seeing cervical injuries and reinjuries in ALS patients, Dr. Steenblock decided to carry out a retrospective study using data from 54 ALS patients he handled from 2011 to 2015 who had a CT scan of their cervical and/or lumbar spine. He found that 52 of the 54 had telltale signs of degenerative pathology and a history of spinal injury and (in many instances) reinjury to the original injury site. An independent radiologist read all the CT scans and reported seeing degenerative changes in the spinal columns of 52 of the 54 ALS patient CT scans "consistent with spinal nerve stenosis-induced injuries (but not spinal cord injuries)".
Steenblock formalized his findings in the form of a paper titled "Hypothesis: Osseous Spinal Injury and Reinjury as a Risk Factor, Biomarker, and Etiological Factor in Sporadic ALS", which was published in the October 2016 issue of the Townsend Letter and is available online.
In the paper, Dr. Steenblock is convinced these bony injuries and reinjuries create tiny breeches or tears in the blood-cerebrospinal fluid (CSF) barrier (whose purpose it is to keep various noxious substances and more from entering the spinal cord).
Over time a number of proinflammatory compounds and other neural cell damaging players are able to penetrate into the spinal cord, along with extracellular calcium. Steenblock also contends that the gut microbiome, which is to say the bacterial and fungal microorganisms in the gastrointestinal tract, fuels the ALS disease process in sufferers. He is, in fact, confident that certain bacteria and fungi in many ALS patients form slimy biofilms which produce free radicals such as superoxide that attract white blood cells (monocytes). The monocytes secrete an enzyme call superoxide dismutase (SOD) which helps disarm superoxide and combat inflammation.
Unfortunately, large numbers of monocytes in people prone to develop ALS or who have developed it flock to biofilms in the gut (and possibly elsewhere) where their internal superoxide dismutase generating machinery gets messed up causing these vital immune cells to make and store misfolded SOD and other noxious molecules. Many of these monocytes then migrate through the tiny tears in the blood-CSF barrier to damaged spinal column areas, where they then dump their essentially neurotoxic cargo (which proceeds to damage motor neurons and initiate or fuel neuron killing pathways).
Hypotheses such as the one advanced by Dr. Steenblock offer an explanation for a observed phenomenon, typically based on limited evidence. They are not conclusive in the "scientifically proven" sense, but rather serve as a starting point for further investigation.
Instead of waiting five or ten years for more research to be done and results to come in, however, Dr. Steenblock has a more practical approach in mind: promote healing of blood-CSF barrier breeches, identify and deal with chronic infections, bust up biofilms as much as possible, chelate out toxic heavy metals where their levels are of concern, and so forth.
He is, for instance, using stem cell-rich bone marrow aspirate concentrate, a wholly legal form of stem cell therapy, to help promote healing of blood-CSF barrier breeches. And while he is armed with insights on how best to combat chronic infections and microbiome issues gleamed from over four decades of in-office clinical work and experimentation, he uses specialized lab tests to reveal infections and possible biofilm involvement, and then introduces specific drug and non-pharmaceutical measures which targets these.
Given enough time, what Steenblock is testing in living ALS patients might make it easier to identify those at risk of developing ALS, as well as provide a clinical algorithm or systematic process for creating customized treatment regimens that delay disease onset and slow progression in those already struggling with this devilish neurodegenerative disease.
Based on material submitted by Dr. Anthony Payne: Copyright 2016, used with permission. – Featured photo by geralt, CC license
Click To Share This Exciting News With Your Friends







Be the first to comment